For SHE Managers & Safety Leaders:
The Case for Doing Emergency Preparedness Better — and Spending Less Doing It
Get your own Action-cards® in our webshop now:
Your organisation may be fully compliant and still be unprepared.
Most safety systems measure training completion. Emergencies measure performance.
Those are not the same thing. You did not get into safety to tick boxes. You got into it because you wanted people to go home unharmed — and you know the difference between a workplace that is genuinely ready and one that merely looks ready on paper.
So here is the question worth sitting with: is your current setup actually working? Not in the records. In practice. When it matters.

The Training Investment That Keeps Losing Value
Most organisations handle preparedness the same way: run a course, issue a certificate, file the record, repeat next year. The problem is not the training itself. It is what happens after — and you know this better than most.
The research puts numbers on something you have likely observed yourself. A review of peer-reviewed literature by the CSA Group found that emergency response skills start declining less than six months after initial training(1).
A 2025 meta-analysis in BMC Public Health confirmed correct performance rates of 74–90% immediately after training, falling markedly within 6 to 8 months(2).
Acute stress compounds this further: it impairs verbal memory, narrows attention, and causes people to rely on far fewer cues than they would in a calm environment(3).
Unaided recall in real emergencies frequently drops below 50% for correct action sequences. This is not a failure of human memory. It is a predictable characteristic of human performance — and it means the system around people needs to be designed accordingly, not the people blamed for it.
What This Costs — in Every Sense
You carry this in two ways simultaneously. The first is the one that keeps you up at night: an incident escalating further than it should because the first response was too slow or simply wrong.
The second matters in budget conversations: OSHA research shows indirect costs — downtime, retraining, management time — are typically 3 to 5 times higher than direct costs(4).
An incident with €50,000 in direct costs may carry a true organisational impact exceeding €200,000.

Better real-world readiness at 30–40% lower total cost does not just save money. It frees resources for more safety. That is not a trade-off — that is a better outcome by every measure.

The Problem With Leaving It to the Designated Few
Many larger organisations invest in a small group of dedicated emergency responders. It is a reasonable instinct — but it rests on an assumption that rarely gets examined: that the designated person will be close enough, and available, when it matters.
Availability is not a guarantee. It is a variable.
Consider what “available” actually means across a normal working week. Lunch break. Different floor. Client meeting. Off sick. On leave. Covering another site. Phone on silent in a training session.
None of these are exceptional circumstances. They are the routine texture of any working day. In organisations running shifts, covering multiple locations, or relying on a small number of designated people, there will be periods — possibly frequent ones — where the effective first response capability of the entire organisation is close to zero.
Most organisations cannot answer a simple question: at any given moment, how far away is the nearest person with the tools and confidence to respond correctly? For many, the honest answer is: we do not know. And on some days, the answer would be uncomfortable.
When minutes matter, proximity is not enough.
But even when the designated responder is present and nearby, the time cost is often unacceptable — and not only in medical emergencies. The research on cardiac arrest makes the underlying principle vivid: survival chances decrease by 10% for every minute without CPR.(5)
The difference between a one-minute response and a four-minute response is not a scheduling preference — it is a 30% reduction in survival probability.(6)
CPR is the most studied example of a principle that applies to any time-critical incident: the faster the correct response, the better the outcome. A chemical spill contained in two minutes causes a fraction of the harm of one left unchecked for ten. A fire reported and acted on immediately is a contained incident; the same fire left while someone locates the designated person is a different situation entirely.
A cyber incident isolated immediately affects one machine; left for ten minutes while someone finds the right person to call, it can compromise an entire network. The unit changes. The principle does not.
Designating a few creates permission for everyone else to wait.
There is a further, subtler problem. Concentrating responsibility in a few designated people gives everyone else implicit permission not to act — what psychologists call the Bystander Effect.(7)
A distributed model, where everyone has the tools and confidence to respond correctly, breaks that dynamic entirely. Action-cards® does not replace the specialist.
It ensures that whoever is actually present in the first critical minutes can act correctly while the specialist is on the way — and that the organisation is never, unknowingly, operating without effective response capability.
A Systemic Solution
Action-cards® are durable, physical emergency response cards — waterproof, shock-resistant, no app or connectivity required — that guide any employee through the correct response sequence step by step, across over 30 sector-specific scenarios.
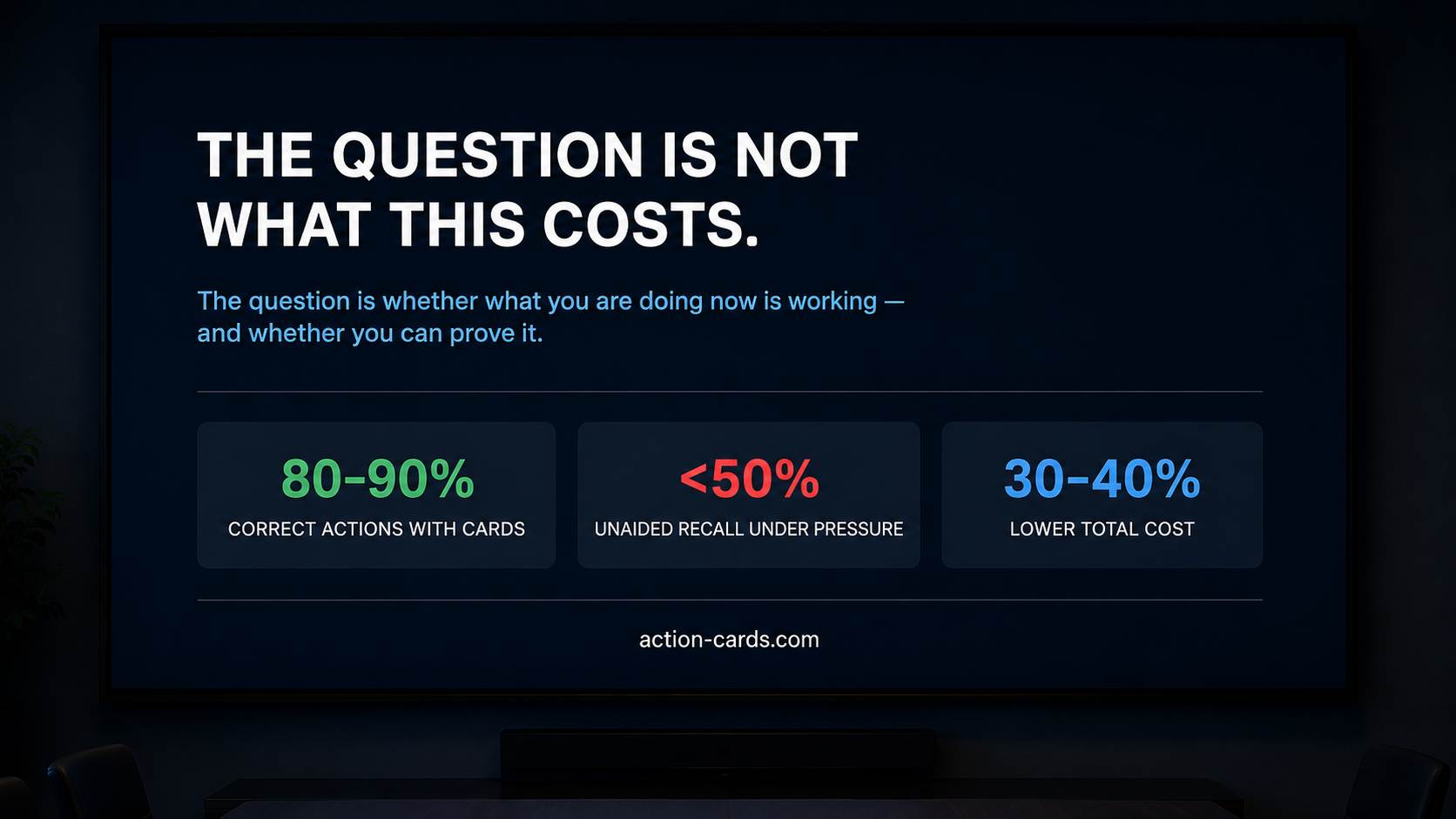
This covers everything from physical first aid and industrial incidents to IT and cyber emergency preparedness, developed with digital security specialists. Internal data shows employees using the cards in realistic scenarios achieve correct action rates of 80–90%. Without them, relying on memory under pressure, performance routinely falls below 50%.

Internal data shows employees using the cards in realistic scenarios achieve correct action rates of 80–90%.
Without them, relying on memory under pressure, performance routinely falls below 50%.
The cards do not just support people in real incidents — they are the guide for ongoing training. Because the correct response sequence is already on the card, any team can run a realistic scenario session themselves. No external instructor needed. No scheduling. No budget line for a trainer.
A team leader picks up the cards, runs a 10–15 minute scenario, and the session is done. This is the structural answer to the forgetting curve — not a bigger training budget, but continuous, self-managed micro-training built into the rhythm of the working week.
AC-Analytics
AC-Analytics (action-cards.com/en/ac-analytics) is where most organisations discover the depth of what they have been missing. Most know who attended training. Very few know who continues to practise — or how well they perform when it counts.
AC-Analytics closes that gap: every QR scan automatically logs time, user, and action, feeding dashboards that surface skill gaps, near-miss patterns, and performance trends across all incident types and locations.
Exportable for compliance, CSR, and insurance conversations in minutes. Your competitors offer training and certification. This offers visibility — and the data to prove that readiness is real, not just recorded.
Most organisations cannot answer a simple question: at any given moment, how far away is the nearest person with the tools and confidence to respond correctly? For many, the honest answer is: we do not know. And on some days, the answer would be uncomfortable.
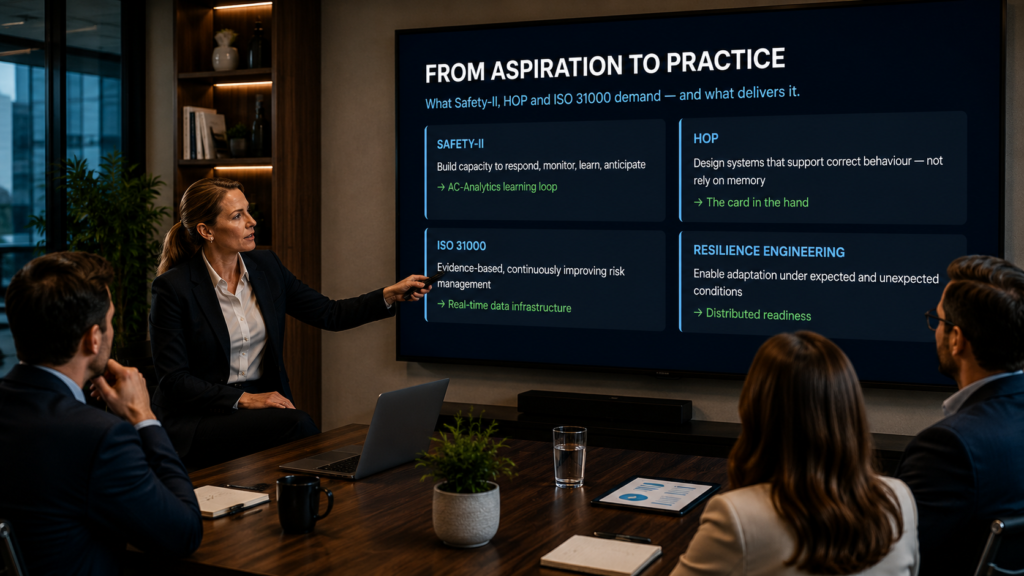
From Framework to Floor
If your organisation has committed to Safety-II, HOP, Resilience Engineering, or ISO 31000, you are probably familiar with a specific frustration: these frameworks are intellectually sound — and genuinely hard to operationalise at the level where emergencies actually happen.
What they share is a common demand: design systems that account for human fallibility rather than demanding perfection from memory; build capacity to respond, monitor, learn, and anticipate; make risk management evidence-based and continuously improving.
Action-cards® is a direct operationalisation of those demands. The cards redesign the context so correct behaviour is supported in the moment — what HOP prescribes. AC-Analytics provides the monitoring, near-miss logging, and learning loop that Safety-II and ISO 31000 require. If the gap between framework aspiration and daily reality has been frustrating, this is what closing it looks like in practice.
The Practical Question
You are responsible for what happens when something goes wrong — whether that is a worker in medical distress, a fire not contained fast enough, or a cyber incident that escalates because no one knows the right first three steps. That responsibility does not end when the certificate is filed.
You are not asking for more money. You are proposing to restructure existing spend to produce better preparedness, better documentation, and measurably better outcomes — across more risk categories, at lower total cost, with the evidence to prove it.
The question is not whether this costs more than what you are doing now. It almost certainly does not. The question is whether what you are doing now is working well enough — and whether you can prove it.
Note:
Action-cards® data on correct action rates (80–90% with cards vs. below 50% unaided) is based on internal performance data collected across customer implementations in realistic training scenarios
Notes
1 CSA Group, First Aid Training and CPR Skills Retention — csagroup.org
2 BMC Public Health, Skill retention after school-based CPR training – a systematic review and meta-analysis (2025) — bmcpublichealth.biomedcentral.com
3 Regehr & LeBlanc, PTSD, Acute Stress, Performance and Decision-Making in Emergency Service Workers, Journal of the American Academy of Psychiatry and the Law (2017); and: Decision-Making During High-Risk Events: A Systematic Literature Review, PMC (2023)
4 OSHA, Safety Pays — Background — osha.gov/safetypays/background
5 Recent advances and controversies in adult cardiopulmonary resuscitation, PMC — pmc.ncbi.nlm.nih.gov/articles/PMC2600120
6 Red Cross / CARES, CPR Facts and Statistics — redcross.org
7 St John Ambulance, From bystander to first responder – the psychology of emergency response — sja.org.uk